

How To Repair An Elevated Diapragm
Introduction [edit | edit source]
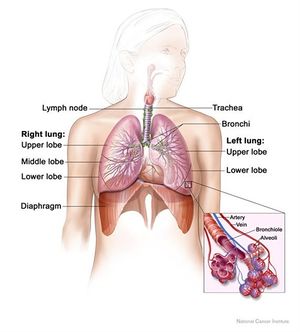
The diaphragm is a double-domed musculoskeletal partitioning separating the thoracic and abdominal cavities.It is crucial for respiration and maintenance of intra-abdominal pressure, and injuries tin result in meaning ventilatory compromise. Traumatic diaphragmatic injuries (TDI) include wounds and diaphragm ruptures due to thoraco-abdominal blunt or penetrating traumas.[1]
Traumatic diaphragmatic injuries are commonly occult and can easily be missed. They occur in a context of multiple trauma making diagnosis difficult.[2] In developing countries where initial care of severely injured patients and diagnostic facilities are less than optimal, blunt TDI may go undiagnosed .[3] An accurate diagnosis requires a high index of suspicion equally missed TDI may result in herniation and strangulation of intra-intestinal viscera into the thoracic cavity .[4] This herniation can interfere with breathing, and blood supply tin can be cutting off to organs that herniated through the diaphragm, dissentious them .[five] In 1579, Paré start described a diaphragmatic rupture in a french arms helm, who initially survived a gunshot wound of the abdomen only died 8 months later of a strangulated gangrenous colon that herniated through a minor diaphragmatic defect the size of a fingertip.[6] It was non until the stop of the nineteenth century that surgical procedures for this condition were existence undertaken. Despite having been recognised early in the history of surgery, blunt traumatic diaphragm rupture was a rarely reported condition before the twentieth century.
Etiology [edit | edit source]
Traumatic diaphragmatic injuries may be acquired past:
- Blunt trauma (route traffic accidents and falls from height are the most common causes[iii] [7])
- Penetrating trauma with direct injury to the diaphragm is more than common and accounts for most two-thirds of cases. It is frequently caused by gunshot injuries, stab wounds or impalement lesions. [8]
- Iatrogenic causes, for case during surgery to the abdomen or chest. .
Clinicians are trained to suspect diaphragmatic rupture, especially if penetrating trauma has occurred to the lower breast or upper abdomen.[9] With penetrating trauma, the contents of the abdomen may not herniate into the chest cavity right away but they may practice so afterward, causing the presentation to be delayed [seven]. Since the diaphragm moves upward and down during breathing, penetrating trauma to various parts of the torso may injure the diaphragm.[10] In extremely rare cases, the patient may have phrenic nerve injury leading to diaphragmatic paralysis.
Incidence and Epidemiology [edit | edit source]
The Incidence of TDI ranges from 0.eight to 8%, simply the true incidence is probable to be higher due to missed or delayed diagnosis.[11]
- Penetrating TDI is highest among thoraco-abdominal gunshot wounds.[12] Information technology accounts for v to ten% of admissions at most trauma centers.[eleven] [13]
- While most blunt TDI are located in the central or posterolateral diaphragm and are related to embryologic weakness, penetrating TDI can occur
anywhere on the diaphragm.[fourteen]
- Right-sided TDI is less common with virtually serial reporting rates of 35-49%, all the same, they are much harder to diagnose due to coverage by the liver, and the true incidence is well-nigh certainly college than reported.[12]
- Left-sided TDI is more mutual, representing 75% of cases.[xv] Information technology take more frequent Injuries to associated organs, and have a higher morbidity and mortality risk.[xiii]
- Bilateral TDI is an extremely rare occurrence, reported as 2 to 8% overall but is seen about exclusively with blunt mechanisms.[xvi]
- Traumatic diaphragmatic injuries can be missed even during exploratory surgery; with ane series demonstrating 14% of TDI missed at an initial laparotomy.[17] This is likely due to the lack of a high alphabetize suspicion and the difficulty with straight visualisation of the hemi-diaphragms [12].
Relevant Anatomy [edit | edit source]
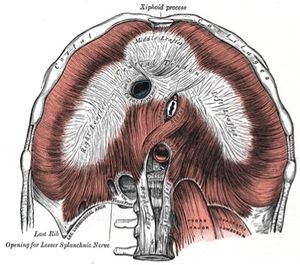
Fig 1: Origin and insertion of Diaphragm
The diaphragm is a bi-domed structure, which separates the contents of the thorax from the intestinal cavity.It is composed of a thin leaflet of cardinal aponeurosis in continuity with peripheral striated muscle, and is divided into ii parts: the lumbar diaphragm and costal diaphragm. It originates anteriorly from the xiphoid, sternum, and the ribs and costal cartilages of ribs 7–12, likewise as posteriorly from the lumbar vertebrae by means of the left and right crura.
The diaphragm inserts into the central tendon which is fused with the pericardium.There are three openings permitting the passage of three big structures.The inferior vena cava and the correct phrenic nerves pass through an opening at the level of T8, the oesophagus and vagus nerves pass through an opening at the level of T10 and the intestinal aorta, thoracic duct and azygous vein pass through an opening at T12.The lumbocostal trigone, a thin expanse of degenerative muscle on the left diaphragm in a higher place the lateral arcuate ligament, represents an embryological transitional region between the costal and lumbar diaphragm.Nerve supply is via the phrenic nerves (C3, C4 and C5) which supplies sensory and motor innervation.Its actions during respiration are responsible for 70% of the work during inspiration.
Muscles of Respiration
Clinical Presentation [edit | edit source]
Clinical presentation varies depending on the mechanism of injury (i.eastward. blunt vs. penetrating) and the presence of associated injuries.[eighteen]
Edgeless traumatic rupture commonly occur in poly-traumatized patient and in near cases, early symptoms are missed, and the injury may exist detected only at exploratory laparatomy for other suspected intra-abdominal organ injuries.[xix]
In the mail-traumatic menstruum, presenting symptoms are unremarkably due to herniation of intra-abdominal organs such as tum, omentum, intestines, spleen and liver into the thoracic crenel.[19] Hence, patients may feel chest pain, recurrent shortness of breath and gastro-intestinal symptoms such as nausea and vomiting, epigastric discomfort or abdominal pains.[iii] Bowel sounds may besides be heard in left-sided hernia associated with bowel loops in the breast.
Commonly associated Injuries are visceral lacerations of the thoracal or intestinal organs and os fractures.For visceral lacerations, splenic ruptures, pulmonary contusion, pneumothorax, liver laceration and cardiac contusion were well-nigh frequent.[20] The most likely associated fractures were pelvic fractures and rib fractures.[21]
Multiple nomenclature systems have been used when referring to the natural history of TDI. An peculiarly appropriate system described by Grimes [22] divides the presentation into three phases,
- the acute phase,The astute phase extends from the fourth dimension of original trauma to the credible recovery from the primary injuries. It is at this phase that the diagnosis of ruptured diaphragm is frequently missed, because of the presence of shock, respiratory insufficiency, visceral injuries and blackout
- the latent phase, information technology begins as the intra-intestinal viscera occupy the defect and variably herniates into the thoracic cavity.
- the obstructive phase. it begins with the signs of visceral obstruction or ischemia as in other hernias.If herniation causes significant lung compression, it tin lead to tension pneumothorax. Diaphragmatic paralysis also may occur. The box beneath depicts the clinical features of the iii phases:[23]
Acute Phase
| Latent Phase
Pain, left shoulder
Abnormal chest 10-ray film findings | Obstructive Stage
|
Diagnosis [edit | edit source]
A timely diagnosis of diaphragmatic injury can be problematic.This is due to other distracting and possibly life-threatening injuries that come up with it. Patients nowadays with daze 50 – 60% of the time.[2] Although delayed diagnosis is common,classical symptoms and signs can atomic number 82 to a speedy diagnosis.
Information on the machinery of injury should be obtained from the patient and pre-hospital care personnel. Concrete findings can exist either thoracic or abdominal.Thoracic signs include decreased jiff sounds,fractured ribs,flail chest,and signs of haemothorax or pneumothorax.
Auscultation of bowel sounds in chest is pathognomic of diaphragmatic rupture,occurring due to herniation of bowel contents.
Abdominal signs include abdominal pain, guarding, absence of bowel sounds, and abdominal swelling, depending on the extent of injuries. Occasionally, physical examination can be relatively normal.
If diagnosis is delayed to months or years after the injury, symptoms are generally less severe,and are due to size reduction in the chest cavity (dyspnoea, orthopnea, respiratory distress), and partial or complete obstruction of herniated intestinal contents (nausea, vomiting, abdominal and chest pain).
The physical signs often present in a diaphragmatic hernia include: - diminished expansion of the chest, damage of resonance, adventitious sounds, cardiac displacement, circulatory collapse, cyanosis, dyspnoea and asymmetry of the hypochondrium.[4]
Radiography
Plain chest radiographs are useful screening tool in cases of suspected diaphragmatic injury. Occasionally, the Chest X-ray can show pathognomic signs of a diaphragmatic injury.[2] Information technology has an unsatisfactory accuracy in detecting TDI; indeed, it may announced normal or it may testify only nonspecific changes in xx – 50% of the patients afflicted by diaphragmatic rupture (Langdorf et al, 2022). Nevertheless, as indicated by Bell and Radswiki,[24] the following signs are helpful in making the diagnosis:
- Inability to trace the normal hemi diaphragm contour
- Intrathoracic herniation of a hollow viscus (tum, colon, small bowel) with or without focal constriction of the viscus at the side of the tear (neckband sign)
- If large, the positive mass consequence may cause a contralateral mediastinal shift
- Visualization of a nasogastric tube above the hemidiaphragm on the left side (as shown in figure 2)
- Left hemidiaphragm much higher than the right
Computerized Tomography (CT) scanning is perchance the nigh useful diagnostic tool in the polytrauma patient. Non just can it provide information about diaphragmatic injuries, but as well reveal other associated injuries. However, the patient does need to be haemodynamically stable. CT offers high accurateness (61% - 87% sensitivity and 72% - 100% specificity) in diagnosing TDI.[25] Helical CT has been shown to improve the early diagnosis of TDI in polytrauma patient. Information technology has a sensitivity of 71% and a specificity of 100%.[26] Conventional CT has a variable sensitivity of between 14 and 61% and a specificity of between 76 and 99%. Multidetector CT allows thinner slicing and more detailed imaging in a shorter time, and a more flexible epitome reconstruction. It is nowadays becoming the imaging modality of choice in trauma patients and also for diagnosing TDI. The findings on CT demonstrating diaphragmatic rupture include:-
· Diaphragm discontinuity or segmental non-recognition.
· Intrathoracic herniation of abdominal contents.
· Constriction of herniated abdominal viscera
· Visualisation of the herniated viscera against the posterior chest wall, the "dependent viscera sign". [27]
Magnetic resonance imaging (MRI) warrants college tissue contrast resolution than CT and enables to clearly depict the diaphragm, but its use in an emergency setting is limited by the longer acquisition times and by the need for patient collaboration. Moreover, the original reward of MRI in comparison with CT in diagnosing TDI i.e its multiplanarity, has been overwhelmed past the evolution of multidetector CT scanners.[28]
Surgical
Considering the difficulty in confirming diaphragmatic injury radiologically, it is unsurprising that the diagnosis is oftentimes unsuspected, and only plant at laparotomy. This can account for the diagnosis of upwardly to fifty% of edgeless ruptures.[2] With the increasing utilisation of laparoscopy and thoracoscopy, more than diaphragmatic injuries are beingness correctly diagnosed and repaired. Diagnostic laparoscopy remains an splendid tool for the detection of haemoperitoneum, solid organ damage and diaphragmatic lacerations.[29]
Complications [edit | edit source]
The most serious complexity of TDI is perforation of viscera into the thoracic cavity, leading to infections like pneumonia, empyemas and subphrenic or intra-abdominal abscesses. To avert this, the vigorous irrigation of the thoracic and abdominal cavity with acceptable drainage is recommended.[thirty] The morbidity includes complications similar suture-line dehiscence, hemi diaphragmatic paralysis secondary to iatrogenic phrenic nerve injuries, respiratory insufficiency, empyemas and subphrenic abscess. The underlying trauma and associated injuries may be the cause of late morbidity.[4]
Management [edit | edit source]
Medical Management [edit | edit source]
First line of direction would focus on resuscitating the patient. Patients with diaphragmatic injury require standard resuscitation and evaluation, including airway control and ventilation equally well every bit restoration of circulation by stopping external haemorrhage and constructive volume restoration. Ensure a patent airway, help ventilation if required, and begin fluid resuscitation if necessary.
Identify an NG tube when possible, every bit this will help in diagnosis if the NG tube appears in the breast on chest radiograph. Aspiration of gastric contents also helps to decompress any abdominal herniation and lessen the abdomino-peritoneal gradient that favors herniation into the breast. Consider placing a chest tube to drain whatsoever associated hemothorax or pneumothorax. Perform this with caution to prevent injury to herniated intestinal contents within the pleural crenel. Most surgeons recommend chest tube placement prior to transfer to another facility. If this is not required immediately in the definitive intendance institution, it may be delayed and completed in the operating room. Performing chest radiography before intubation may yield a improve result (because it is more likely to testify associated herniation).[18]
Surgical Management [edit | edit source]
Surgical repair via laparatomy or thoracotomy is necessary, even for small tears, because the defect volition not heal spontaneously. Astute cases of TDI are better managed via a laparatomy as this also rules out and treat associated intra-abdominal organ injuries. Delayed cases, however, are better managed via a thoracotomy or thoraco-abdominal approach because of intra-thoracic adhesions.[31] Repair of diaphragmatic defect is commonly accomplished with interrupted not-absorbable sutures like nylon and prolene in a single or double-layered fashion. Mesh repair is used for large defect.
Physiotherapy Direction [edit | edit source]
Assessment [edit | edit source]
Following Laparatomy and thoracotomy, at that place is overwhelming evidence of changes in lung function and associated clinical manifestations. These changes include feature reduction in lung volume which is primarily restrictive in nature, reduction in functional residual capacity, slowing of mucociliary clearance, and abnormalities in gaseous exchange.[32] Other frequently observed postoperative complications are mail-thoracotomy pain syndrome and ipsilateral reduction in upper extremity range of motion and strength.[33]
Cess is primarily focused on physical examination, chest expansion ABG analysis, pulmonary function exam, breast X-ray, SpO2 (oxygen saturation), peripheral musculus strength and cardiopulmonary practice testing.[34] In the preoperative phase, concrete exam should address the presence of dyspnoea, exercise tolerance, coughing, and expectoration. Examination should as well focus on respiratory charge per unit, blueprint of breathing, and wheezing. Patient may show either normal or altered breathing pattern on physical examination. Postoperatively, patients ordinarily nowadays with monotonous shallow breathing without spontaneous deep breaths, increase in respiratory rate, decreased tidal volume, and significant modify in minute ventilation. Wheeze, rales, or prolonged breath sounds will be revealed on auscultation.
Aims of Intervention [edit | edit source]
Generally the main aims in the postoperative phase are to maintain adequate ventilation, to assistance in the removal of any excess lung secretions and to help in the full general positioning, bed mobility and early on ambulation of the patient. Prevention of reduced joint movements or poor posture secondary to incisions or tubes, monitoring of adequate pain relief and appropriate oxygen therapy and humidification are too very of import.
Physiotherapy Techniques [edit | edit source]
Physiotherapy techniques which help to accomplish these aims include:
Early on mobilization : With the evolution of laparoscopic surgery, improved anaesthetic and hurting management many patients are ofttimes able to mobilize independently from a very early stage postoperatively. Some patients volition require assist because of the presence of the diverse drips and drains and it is sometimes safer to have two people assisting for the first stand or walk considering of the patient's full general fatigue and the adventure of postural hypotension. A graduated walking plan adapted to suit each patient should be encouraged with the introduction of stair climbing at an appropriate stage. Hanekom et al [35] reported early mobilization to be a beneficial intervention for patients post-obit upper abdominal surgeries. It is established that delaying early mobilization caused an increment in post-operative pulmonary complications.[36]
Breathing Exercises: Deep breathing exercises are taught to the patients and tin can help to obtain full expansion of the breast wall during spontaneous breathing. This is essential to help restore lung office and to prevent subsequent chest deformity. The patient is instructed to relax the shoulder and upper chest, take a irksome deep breath in through the nose to fill upward the lungs as fully as they can, hold breath for a few seconds (three seconds), and breathe out slowly through the oral cavity. This should be washed five times every 60 minutes. Patients are encouraged to practice animate exercise frequently even when physical therapist isn't present.
Incentive spirometry
Agile cycle of breathing (ACBT)
Thoracic expansion exercises
Cough and Huffing Technique
Transcutaneous electrical nerve stimulation (TENS): TENS is a non-invasive analgesia technique that produces a significant reduction in pain. The apply of TENS has been shown to decrease pain from shoulder flexion in patients undergoing axillary thoracotomy.[37]
Conclusion [edit | edit source]
Traumatic injuries of the diaphragm are often hidden and tin can be masked by other violent injuries associated with polytrauma. A high index suspicion and the use of relevant radiological investigation should aid in early diagnosis. Mobilization, deep breathing exercise, thoracic expansion practise should too be integrated early on into patients care.
References [edit | edit source]
- ↑ Thiam O, Konate I, Gueye ML, Seck Yard, Cisse M, Diop B, Dirie ES, Ka O, Thiam M, Dieng M, Dia A. Traumatic diaphragmatic injuries: epidemiological, diagnostic and therapeutic aspects. Springerplus. 2022 Dec;five(1):1-half-dozen.
- ↑ 2.0 ii.1 2.two 2.3 Bosanquet D, Farboud A, Luckraz H. A review diaphragmatic injury. Respiratory medicine CME. 2009;two(i):ane-half-dozen.
- ↑ 3.0 3.1 3.2 Kidmas AT, Iya D, Isamade ES, Ekedigwe Eastward. Delayed presentation of blunt traumatic diaphragmatic hernia: a example report. Nigerian periodical of surgical inquiry. 2005;7(3):323-four.
- ↑ iv.0 four.1 iv.2 Petrone P, Leppäniemi A, Inaba Grand, Søreide K, Asensio JA. Diaphragmatic injuries: challenges in the diagnosis and management. Trauma. 2007;9(4):227-36.
- ↑ Senent-Boza A, Segura-Sampedro JJ, Olivares-Oliver C, Padillo-Ruiz FJ. Hepatothorax Caused by a Late Mail-Traumatic Diaphragmatic Rupture. Cirugía Española (English language Edition). 2022;ix(93):e101.
- ↑ Bhatia S, Kaushik R, Singh R, Sharma R, Attri A, Dalal U, Dalal A, Bansiwal R. Traumatic diaphragmatic hernia. Indian Journal of Surgery. 2008;seventy(2):56.
- ↑ seven.0 7.1 Scharff JR, Naunheim KS. Traumatic diaphragmatic injuries. Thoracic surgery clinics. 2007;17(1):81-five.
- ↑ Morgan BS, Watcyn-Jones, T, Garner JP. Traumatic diaphragmatic injury. Journal of the Royal Ground forces Medical Corps. 2010;156(3):139-144.
- ↑ Asensio JA, Roldán Thousand, Petrone P, Rojo E, Tillou A, Kuncir E, Demetriades D, Velmahos Thou, Murray J, Shoemaker WC, Berne Telly. Operative direction and outcomes in 103 AAST-OIS grades Four and V circuitous hepatic injuries: trauma surgeons nevertheless demand to operate, but angioembolization helps. Periodical of Trauma and Acute Intendance Surgery. 2003;54(iv):647-54.
- ↑ Fleisher GR, Ludwig S, editors. Textbook of pediatric emergency medicine. Lippincott Williams & Wilkins; 2010.
- ↑ 11.0 11.1 Lopez PP, Arango J, Gallup TM, Cohn SM, Myers J, Corneille M, Stewart R, Paring DL. Diaphragmatic injuries: what has changed over a twenty-twelvemonth period?. The American Surgeon. 2010;76(5):512-6.
- ↑ 12.0 12.1 12.2 DeBarros Grand, Martin MJ. Penetrating traumatic diaphragm injuries. Current Trauma Reports. 2022;1(2):92-101.
- ↑ thirteen.0 xiii.1 Zarour AM, El-Menyar A, Al-Thani H, Scalea TM, Chiu WC. Presentations and outcomes in patients with traumatic diaphragmatic injury: a 15-year experience. Journal of Trauma and Acute Intendance Surgery. 2022;74(six):1392-8.
- ↑ Dirican A, Yilmaz Yard, Unal B, Piskin T, Ersan 5, Yilmaz Southward. Astute traumatic diaphragmatic ruptures: a retrospective study of 48 cases. Surgery today. 2022;41(x):1352.
- ↑ Hanna WC, Ferri LE. Acute traumatic diaphragmatic injury. Thoracic surgery clinics. 2009;19(iv):485-ix.
- ↑ Ties JS, Peschman JR, Moreno A, Mathiason MA, Kallies KJ, Martin RF, Brasel KJ, Cogbill Thursday. Evolution in the management of traumatic diaphragmatic injuries: a multicenter review. Journal of Trauma and Acute Care Surgery. 2022;76(4):1024-8.
- ↑ Esme H, Solak O, Sahin DA, Sezer Grand. Blunt and penetrating traumatic ruptures of the diaphragm. The Thoracic and cardiovascular surgeon. 2006;54(05):324-seven.
- ↑ eighteen.0 18.1 Welsford. 2022. [online] Emedicine.medscape.com. Available at: https://emedicine.medscape.com/article/822999-treatment [Accessed 15 Feb. 2022]
- ↑ 19.0 19.ane Mercadante E, De TG, Rendina EA, Venuta F, Moretti M, Aratari MT, Furio GC. Diagnostic delay in post-traumatic diaphragmatic ruptures. Minerva chirurgica. 2001;56(3):299-302.
- ↑ Hofmann S, Kornmann Thousand, Henne-Bruns D, Formentini A. Traumatic diaphragmatic ruptures: clinical presentation, diagnosis and surgical approach in adults. GMS Interdisciplinary plastic and reconstructive surgery DGPW. 2022;1.
- ↑ Pantelis D, Burger C, Hirner A, Wolff, M. Indirect Traumatic Diarrheal Rupture. The Surgeon. 2006;77 (4):360-366
- ↑ Grimes OF. Traumatic injuries of the diaphragm: Diaphragmatic hernia. The American Journal of Surgery. 1974;128(2):175-81.
- ↑ Shah R, Sabanathan S, Mearns AJ, Choudhury AK. Traumatic rupture of diaphragm. The Annals of thoracic surgery. 1995;60(5):1444-ix.
- ↑ Bell, D. and Radswiki. Diaphragmatic rupture. [online] Radiopaedia.org. 2022. Available at: https://radiopaedia.org/articles/diaphragmatic-rupture [Accessed 15 Feb. 2022]
- ↑ Panda A, Kumar A, Gamanagatti S, Patil A, Kumar S, Gupta A. Traumatic diaphragmatic injury: a review of CT signs and the deviation betwixt blunt and penetrating injury. Diagnostic and interventional radiology. 2022 ;20(two):121.
- ↑ Iochum S, Ludig T, Walter F, Sebbag H, Grosdidier G, Blum AG. Imaging of diaphragmatic injury: a diagnostic challenge?. Radiographics. 2002;22(suppl_1):S103-16.
- ↑ Sangster G, Ventura VP, Carbo A, Gates T, Garayburu J, D'Agostino H. Diaphragmatic rupture: a frequently missed injury in blunt thoracoabdominal trauma patients. Emergency radiology. 2007;13(5):225-30.
- ↑ Bonatti Yard, Lombardo F, Vezzali North, Zamboni GA, Bonatti G. Blunt diaphragmatic lesions: Imaging findings and pitfalls. World journal of radiology. 2022;viii(ten):819.
- ↑ Asensio JA, Petrone P. Diaphragmatic injury. Current surgical therapy. 8th ed. Philadelphia: Elsevier Mosby Co. 2004:946-55.
- ↑ Yilmaz M, Isik B, Ara C, Yilmaz S, Kutlu R, Kocak Ö, Ugras Grand, Kirimlioglu Five. Gastric perforation during breast tube placement for acute diaphragmatic rupture and review of the literature. Injury Extra. 2006;37(ii):71-5.
- ↑ Edino ST, Alhassan S, Ajayi OO. Traumatic diaphragmatic rupture with gastro-pleuro-cutaneous fistula: A example report and literature review. Nigerian J Surg. 2002;8:eighteen-20.
- ↑ Reeve J.2008. Physiotherapy interventions to prevent postoperative pulmonary complications post-obit lung resection. What is the evidence? What is the practice?.
- ↑ Belda J, Cavalcanti M, Iglesias M, Gimferrer JM, Torres A. Respiratory infections after lung cancer resection. Clinical Pulmonary Medicine. 2006;13(one):8-16.
- ↑ Sultanpuram Due south, Alaparthi GK, Krishnakumar SK, Ottayil ZC. Physiotherapy practise patterns for direction of patients undergoing thoracic surgeries in Bharat: a survey. Surgery research and practice. 2022;2016.
- ↑ Hanekom, S.D., Brooks, D., Denehy, L., Fagevik-Olsén, Grand., Hardcastle, T.C., Manie, S. and Louw, Q., 2022. Reaching consensus on the physiotherapeutic management of patients post-obit upper abdominal surgery: a pragmatic approach to translate equivocal prove.BMC medical information science and decision making,12(ane), p.five.
- ↑ Haines KJ, Skinner EH, Berney S, Austin Wellness Post Study Investigators. Association of postoperative pulmonary complications with delayed mobilisation following major abdominal surgery: an observational accomplice study. Physiotherapy. 2022;99(2):119-25.
- ↑ González PE, Novoa NM, Varela G. Transcutaneous Electric Nervus Stimulation Reduces Post-Thoracotomy Ipsilateral Shoulder Pain. A Prospective Randomized Study. Archivos de Bronconeumología (English Edition). 2022;51(12):621-half-dozen.

How To Repair An Elevated Diapragm,
Source: https://www.physio-pedia.com/Physiotherapy_Management_of_Traumatized_Diaphragm
Posted by: kratzolonstake90.blogspot.com
0 Response to "How To Repair An Elevated Diapragm"
Post a Comment